
| Received | : | Dec 10, 2019 |
| Accepted | : | Feb 12, 2020 |
| Published Online | : | Feb 14, 2020 |
| Journal | : | Journal of Abdominal Wall Reconstruction |
| Publisher | : | MedDocs Publishers LLC |
| Online edition | : | http://meddocsonline.org |
Cite this article: Kallinowski F, Nessel R, Gorich J, Grimm A, Loffler T. CT Abdomen with Valsalva’s maneuver facilitates grip-based incisional hernia repair. J Abdom Wall Reconstr. 2020; 2(1): 1006.
Background: Grip-based incisional hernia repair needs the accurate determination of the hernia defect area and of the distensibility of the hernia area. Both parameters can be derived using computerized tomography of the abdomen at rest and during Valsalva’s maneuver. The two existing ways of analysis are compared for the first time on ten patients in a prospective observational study.
Objective: To develop a reliable and objective assessment of the hernia size and the distensibility of the abdominal wall prior to ventral hernia repair comparing two previously published methods in a prospective observational study. Methods: Consecutive patients scheduled for repair of incisional hernia were included. The CT scan of the abdomen was intended to determine the hernia size and the area of instability of the abdominal wall preoperatively. The scans were evaluated by five different observers (technician, radiologist, surgeons) using two different ways previously reported in the literature.
Results: In all ten patients, new information was generated significantly changing the incisional hernia repair. Basically, both evaluation methods yielded the same results with one being more consistent. Further analysis of the more consistent method demonstrated marked variations upon multiple readings both with one and with multiple observers. After 12 observations, the variation stays below 5 % even in the most unstable abdominal walls. With elevation of the abdominal pressure, the hernia defect area increased by 10 % with the hernia sac volume widening up to fivefold, on the average.
Conclusions: Grip-based incisional hernia repair critically depends on the mesh: defect area ratio and on the distensibility of the abdominal wall. Both parameters can be reliably assessed using computerized tomography of the abdomen at rest and with Valsalva’s maneuver using more than 12 observations. The application of intravenous contrast can be omitted for the acquisition of data.
Keywords: Hernia repair; Abdominal wall; Valsalva’s maneuver
Incisional hernia is a frequent consequence of major surgery causing pain and disability and likes to recur frequently. Biomechanically stable repair of the abdominal wall reduces both pain and recurrence after one year [1]. Variables necessary to construct a biomechanically stable abdominal wall such as the hernia area are identified by imaging procedures. Imaging can further guide in deciding between treatment options in difficult cases [2]. So far, Computerized Tomography (CT) of the abdomen is the only modality which is evaluated to some extent. Two different approaches have been reported for the analysis of the abdominal and/ or the intraperitoneal volumes concurrent with the sac volumes of the incisional hernias [3,4]. A comparison between the approaches is lacking. Here, we report for the first time an analysis of 10 patients investigated for abdominal pain with concurrent incisional hernias comparing both approaches.
Valsalva’s maneuver has been reported to increase the diagnostic accuracy of CT of the abdomen for incisional hernia [5,6]. Using Valsalva’s maneuver, additional important influences on the biomechanical stability of ventral hernia repair can be assessed: changes of the size of the hernia upon pressure loading necessary for the calculation of the mesh: defect area ratio and the distension or even the elasticity of the abdominal wall [7,8]. Here, we report for the first time the corresponding calculations on 10 consecutive patients.
We investigated 10 consecutive patients with abdominal pain and incisional hernia. The basic clinical parameters are given in Table 1. The protocol for CT scanning was derived from the low-dose, no contrast protocols searching kidney stones. All CT imaging data have been collected without contrast medium on deep inspiration in a two step technique. Following the scout for planning, two CT examinations in a sequential acquisition mode (slice thickness 0.6 mm, 110 - 130 kV) of the whole abdomen from the diaphragm to the symphysis were performed: first in relaxation with the abdomen at rest, than with the patient straining oneself with Valsalva’s maneuver as a second step. Examination time was less than 30 seconds using a Somatom 16 Scanner (Siemens, Erlangen, Germany). The changes of the abdominal, the peritoneal and the hernia sac volumes were used to calculate the distensibility of the tissues.
Table 1: Clinical parameters of the patients investigated. BMI: Body Mass Index, ASA: Amercian Society of Anaesthesiologists Classification
From each scan, an evaluation was performed as given previously [3,4] and depicted in figures 1 and 2. This was repeated by all five observers one to three times to assess the individual and interobserver differences. One observer evaluated all scans repeatedly using the same methodology in three consecutive weeks to assess the intraobserver variation. The same observer evaluated all scans repeatedly up to 26 times in one session to assess the variation upon repeated measurements.
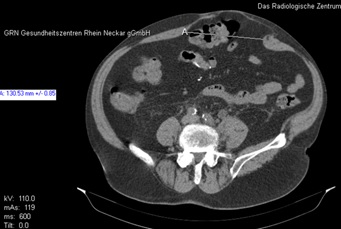

and during Valsalva’s maneuver (right) derived from a patient with
an incisional hernia were used for evaluation. “A” and “Distanz”
indicate the hernia diameter in the transverse projection.")
Figure 1: Corresponding slices of a CT abdomen at rest (left) and during Valsalva’s maneuver (right) derived from a patient with an incisional hernia were used for evaluation. “A” and “Distanz” indicate the hernia diameter in the transverse projection.
 and of the peritoneal volume as the
layer of a sphere, [4] with the corresponding hernia sac volume as
half of an ellipsoid based on the hernia defect area (bottom).")
Figure 2: Geometrical assumptions used for the calculation of the abdominal volume and the corresponding hernia sac volume both as an ellipsoid [3] (top) and of the peritoneal volume as the layer of a sphere, [4] with the corresponding hernia sac volume as half of an ellipsoid based on the hernia defect area (bottom).
From the measurements, volumes were calculated as a rotational or skewed ellipsoid or as a spherical layer according to the models given by Tanaka et al. [3] and by Sabbagh et al. [4]. The first method calculates an ellipsoid for both the abdominal and hernia sac volume. The latter procedure represents the peritoneal volume as a layer of a sphere with the hernia volume being half of an ellipsoid (for further description see Figure 2). In our application, the volumes of the liver was excluded. The varying volume of the urinary bladder was included. All data were accumulated into Excel spreadsheets and analyzed using the inbuilt statistical and graphical functions. Statistical parameters were calculated online using standard parametric and nonparametric statistics as needed.
Upon Valsalva’s maneuver, the abdominal, the peritoneal and the hernia sac volume changed (figure 1). In all patients, the planned clinical procedure was changed after the CT scan of the abdomen with Valsalva’s maneuver (Table 2). In each case, the area of abdominal instability increased upon the exertion of Valsalva’s maneuver. Major changes addressed the biomechanical stability of the intended incisional hernia repair [1,7,8]. The hernia area changed upon Valsalva’s maneuver by almost 50 % using Tanaka’s method [3] from an average of 126 + 121 cm2 to 176 + 143 cm2 after Valsalva’s maneuver. Using Sabagh’s method [4], the change of the hernia area was reduced to 10 % varying between 132 + 110 cm2 at rest and 145 + 106 cm² after Valsalva’s maneuver. In figure 1, one of the diameters used to calculate the volumes according to Sabbagh et al. [4] is depicted for patient number 4. Due to muscular contraction the diameter shrinks in this case from 13 to 11.8 cm decreasing both the area of the half ellipsoid representing the hernia sac and the cover plate of the slice of a sphere representing the peritoneal volume [4]. In contrast, the length of the center line of a throught ellipsoid representing the hernia sac volume stays constant and is unrelated to the abdominal volume calculated according to Tanaka et al [3].
Table 2: Clinical consequences of the CT abdomen at rest and after Valsalva’s maneuver for the patients investigated.
Since the mesh: defect area ratio is critical for the calculation of the grip necessary for a biomechanically stable hernia repair further differences between the results of Tanaka’s [3] and Sabbagh’s [4] procedures were sought after. First, both the abdominal [3] and the peritoneal [4] volumes were related to the body mass index of the patients with the correlation of the peritoneal volume being somewhat higher (abdominal volume: r = 0.445, p= 0.197; peritoneal volume: r = 0.603, p = 0.065; Figure 3). As expected, the abdominal volume was significantly higher as compared with the peritoneal volume (6146 + 2802 cm3 versus 3363 + 1343 cm3, p = 0.00057; fig. 4). In our data, the abdominal volume was found to be closely correlated to the peritoneal volume (r = 0.90117, p = 0.00037). The hernia sac volume was found to be similar with both calculations and unrelated to the abdominal or peritoneal volume (410 + 1165 cm3 versus 411 + 538 cm3, p = 0.308; Figure 4). Again, both methods gave very closely correlated results for the hernia sac volumes at rest (r = 0.91256, p = 0.00023). Since all parameters were closely related at rest but the hernia area was less variable with the calculation method according to Sabbagh et al. [4] this method was used in the following analysis.
.jpg "Figure 3: Abdominal (dots) and peritoneal (circles) volumes as
a function of the body mass index. Abdominal volumes were calculated as ellipsoids [3]. The peritoneal space was computed using
a spherical layer [4].")
Figure 3: Abdominal (dots) and peritoneal (circles) volumes as a function of the body mass index. Abdominal volumes were calculated as ellipsoids [3]. The peritoneal space was computed using a spherical layer [4].
.jpg "Figure 4: Abdominal (white) and peritoneal (black) volumes
with the corresponding hernia sac volumes at rest (white and
black boxes)")
Figure 4: Abdominal (white) and peritoneal (black) volumes with the corresponding hernia sac volumes at rest (white and black boxes)
Assessing the changes of the volumes upon Valsalva’s maneuver, less variation was observed with the peritoneal volume as compared with the hernia sac volume (Figure 5). The hernia sac distended up to 5 fold whereas the abdominal volume shifted by an average of 11 % when summing up all distension observations. The variation between observers was independent from hernia volumes. In 20 % of all observations, the hernia sac appeared to shrink upon Valsalva’s maneuver which was due to a selection bias or due to muscular contraction when taking corresponding slices of the CT scans. Assessing the individual variations of each observation between observers in this way, the hernia sac volume varied to an larger extend as compared with the peritoneal volume (Figure. 6). A single observation can differ by 150 % assessing the distension of the hernia sac and by 100 % analyzing the peritoneal volume. Again, most of the variation is caused by the varying selection of scan between different observers. In comparison, the intraindividual variation is somewhat smaller being more pronounced with the peritoneal volume (Figure 7).

Figure 5: : Intra-observer variation of the volumes obtained from 10 different patients. One observer rated four times in one session and repeated this three times in weekly intervals.
Hernias with larger areas of unstable abdominal wall segments and /or with muscular diastasis seem to be more prone to this phenomenon. An example is given in a patient with a recurrent incisional hernia (Figure 8). The instability of the abdominal wall extends to the left far beyond the hernia diameter given by the white line which extends from 9.6 cm on the left panel to 10.6 cm on the right panal with Valsalva’s maneuver. In this way, the hernia sac extends beyond the diameter of the hernia orifice which increased only about 10 % upon pressure. Different observers varied largely in this case both in hernia area, hernia volume and tissue distension. Similar phenomena occurred in the other patients with recurrent hernias and / or large instability of the abdominal wall.
 and after Valsalva’s maneuver (right). The metal tacks
in the right-sided abdominal wall indicate the extent of the intraperitoneal onlay mesh used for the previously attempted repair.")
Figure 8: Variation of the shape of a recurrent incisional hernia at rest (left) and after Valsalva’s maneuver (right). The metal tacks in the right-sided abdominal wall indicate the extent of the intraperitoneal onlay mesh used for the previously attempted repair.
In both stable and unstable abdominal walls, variation dropped rapidly with increasing numbers of observations (figure 9). After 4 observations in cases with unstable abdominal walls, the variation of the measurements decreased from 150 to 30 % with virtual no variation after 12 observations. Taking 12 measurements and calculating the corresponding volumes took on the average 21 + 2 minutes. Assessing stable abdominal walls, differences between measurements were below 5 % after 4 observations already. In all cases, the assessment of hernia base area or hernia volume changes can be used to assess the tissue distension as a measure of tissue elasticity which can be directly related to the grip necessary for a durable incisional hernia repair.

Figure 9: : Inter-observer variation of the volumes obtained from 10 different patients as a function of the accumulated ratings arbitrarily dividing between patients with more stable and more unstable abdominal walls. One observer rated four times in one session and repeated this three times in weekly intervals. Five observers rated between once and twenty-six times in one session.
Area and volume measurements of abdomen, peritoneum and hernias were performed increasingly since the last 10 – 15 years mostly using CT scans before performing complex procedures [9-12]. Volumes were investigated at rest with researcherbased [3,4,9,12] and manufacturer-given procedures [10,11].
In manufacturer-given algorithms, experienced researchers are required to label anatomical landmarks which can take an hour and more out of the human resource [11]. Accumulated pixels, voxels or segmentation procedures can make calculations precise to a fraction of the cubic millimeter but clinically, shiftable organs such as liver, kidneys or bowel and fixed structures such as spine, pelvis or organs with variable filling such as the urinary bladder give rise to larger variation in the results yet neglected in the analysis. Since researcher-based methods are performed faster – in our hands 21 minutes for 12 ratings – and potentially more applicable to middle- and low-income countries where fancy software algorithms are unaffordable we decided to proceed with the analysis of the researcher-based evaluation of parameters related to incisional hernia repair.
Researcher-based models can be divided by two basic principles first described by Tanaka et al. [3] and Sabbagh et al. [4]. The first aims at the description of an ellipsoid-shaped hernia sitting on an ellipsoid abdomen and the latter considers the hernia as half of an ellipsoid sitting on a peritoneal cavity with the shape of a slice of a sphere. Since both models give the same information (Figure 3) differences were sought after. First, the abdominal volume was always higher than the peritoneal volume (Figure 4). Secondly, the variation was lower with the model used by Sabbagh et al. [4]. Since the grip-based incisional hernia repair requires a precise assessment of the hernia area [7,8] the latter model was better suited for the grip-based ventral hernia repair.
At the beginning, CT was used to assess whether the use of progressive pneumoperitoneum was indicated [9]. Recently, preoperative computed tomography at rest and during Valsalva’s maneuver was used to assess retrospectively whether a more complex procedure such as a component separation might have been necessary [14]. In our prospective study, the precise hernia size and the distensibility of the abdominal wall was used to calculate the grip to be achieved during surgery in order to create a biomechanically stable incisional hernia repair [7,8]. Patients repaired with sufficient grip exhibit so far no recurrences after one year and do not require pain medications [15]. Since the distensibility of the hernia sac volume is generally higher than the distension of the abdominal wall the grip calculation should account for this in the future.
Using the Valsalva’s maneuver increased the detection of small hernias indicating an unstable abdominal wall in 4 out of 10 patients (Table 1, 2). Besides this, the maneuver critically influences the mesh: defect area ratio which is the basis for the calculation of grip values [15,16]. Since an unstable abdominal wall markedly influences the distension of the peritoneal and of the hernia sac volume an abdominal CT scan for an incisional hernia should always be augmented with a Valsalva’s maneuver.
The inter- and intra-observer variation influences the values obtained (Figure 6 & 7). Multiple readings should be mandatory before a certain value of the abdominal, peritoneal or hernia sac volume or of the hernia base area can be given with little variation (Figure 9). It still has to be shown that machine-driven algorithms using segmentation can decrease the amount of variation [11,14]. Since the anatomical landmarks are added by hand by an experienced researcher segmentation takes at least one hour of valuable expert time, is open to human error as well and requires specialized software [11]. The approach we used here can be applied anywhere and might not be too expensive for low- and middle-income countries or hospitals. Specialized software might not be available in rural areas but seems to be dispensable as demonstrated by our group of surgeons, technicians and specialized radiologists.

Figure 6: Inter-observer variation of the volumes obtained from 10 different patients. Each observer rated between one and twelve times.

Figure 7: Intra-observer variation of the volumes obtained from 10 different patients. One observer rated four times in one session and repeated this three times in weekly intervals.
Both inter- and intra-observation vary markedly on the single acquisition of data but 10-12 observations generally brings the variation below 5 % both in stable and unstable abdominal walls (Figure 9). With this approach, the human sampling error is minimized. Technical variation such as a shift of the region of interest out of the corresponding slice of the CT scan has been estimated to vary between 0 and 2 cm in the various regions of the abdomen such as subxiphoidal, periumbilical or above the symphysis. Future approaches will most probably include artificial intelligence to automatically perform segmentation or tensor calculations of continuum mechanics to assess the torsion gradients within the abdomen and the hernia sac upon Valsalva’s maneuver. The latter approach is now in the state of bench testing [17,18]. Recently, the term “loss of domain” was standardized using Sabbagh’s method [4,19] Applying this definition, the wide inter-observer and intra-observer variation has to be recognized and multiple readings are recommended before a patient is triaged to a treatment plan.
CT abdomen with Valsalva’s maneuver should be mandatory before attempting incisional hernia repair since the procedure detects unstable abdominal walls. The peritoneal cavity should be assessed as a layer of a sphere with the hernia sac being considered one half of an ellipsoid. The hernia area varies with the application of pressure assessing the tissue elasticity. A total of 4 observations are the lowest number of repetition with a stable abdominal wall. With an unstable abdominal wall, 10 – 12 observations are enough for the assessment of the hernia area and of the distensibility of the abdominal wall.
We always work towards offering the best to you. For any queries, please feel free to get in touch with us. Also you may post your valuable feedback after reading our journals, ebooks and after visiting our conferences.

